The Correct Answer is e
The Poiseuille-Hagen formula is the mathematical expression of the relation between the flow in a long narrow tube, the viscosity of the fluid & the radius of the tube.
F = (PA – PB) x p x 1 x r4
8 h L
Where:
F = flow;
PA – PB = pressure difference between the 2 ends of the tube;
h = viscosity;
r = radius of tube;
L = length of tube;
Since flow is equal to pressure difference divided by resistance,
R = 8hL
pr4
ie. flow varies directly & resistance inversely with radius to power of 4.
\ blood flow is affected markedly by small changes in calibre of vessels.
If, for example, there is:
19% increase in radius of blood vessel Þ
flow thru a vessel is doubled;
when radius is doubled, resistance is reduced to
6% of its previous value.
This is why organ blood flow is so effectively regulated by small changes in calibre of arterioles.
The Correct Answer is d
After capillary beds blood is collected in venules which are tributaries of veins. These vessels provide a low pressure blood reservoir through which blood returns to the heart.
The Correct Answer is a
Windkessel in German means elastic reservoir. The Windkessel effect is the recoil effect during diastole of vessel walls that have been stretched during systole Þ it is because of this recoil that forward flow is continuous during diastole.
Answer: AC
DISCUSSION: It is generally held that patients with a diagnosis of acute appendicitis should receive antibiotics such as cefoxitin or cefotetan. Administration can be discontinued after 24 hours if the appendix is not gangrenous or ruptured. Multiple antibiotics are unnecessary in straightforward cases.
Answer: C
DISCUSSION:
It is very difficult to establish a firm diagnosis of acute appendicitis in an infant of 1 year or younger since the patient cannot provide a history or be helpful during the physical examination. It is rare to make a definitive diagnosis preoperatively in such infants, and in such cases the appendix is usually perforated at the time of operation. While appendicitis is somewhat more difficult to diagnose in the elderly because of the reduced response to inflammation; nevertheless, it is usually possible to make the diagnosis. With pregnant women it is wise to remember that the enlarging uterus in the last trimester dislocates the appendix higher in the abdomen and that the signs and symptoms follow this anatomic shift accordingly.
Answer: C
DISCUSSION:
The majority of patients with acute appendicitis have an obstructed lumen that is due to either hyperplasia of the lymph follicles in the wall of the appendix or a fecalith. The obstruction creates a site where the bacteria in the lumen multiply rapidly, producing exotoxins and endotoxins that then ulcerate the mucosa, allowing pathogenic organisms to enter the wall of the appendix. An inflammatory process follows that can extend to the serosa, and penetration through the serosal layer causes generalized peritonitis.
Answer: A-TRUE, B-TRUE, C-FALSE, D-TRUE
DISCUSSION: Mesenteric cysts are most often due to congenital lymphatic spaces that gradually enlarge as they fill with lymph. They generally present as abdominal masses accompanied by pain, nausea, and vomiting. They usually can be diagnosed by physical examination and have characteristic lateral mobility. They are best treated by surgical excision, and intestinal resection may be necessary for complete removal. Omental cysts are frequently asymptomatic but may present with vague discomfort or as a mobile abdominal mass that can cause torsion of the omentum. Torsion generally presents with signs and symptoms compatible with acute cholecystitis, appendicitis, or a twisted ovarian cyst. Treatment entails local resection.
Answer: C
DISCUSSION: Peritonitis is inflammation of the peritoneum and can be septic or aseptic, bacterial or viral, primary or secondary, acute or chronic. Most surgical peritonitis is secondary to bacterial contamination from the gastrointestinal tract. Primary peritonitis refers to inflammation of the peritoneal cavity without a documented source of contamination. It is more common in children than in adults and in women than in men. The female predominance is felt to be explained by entry of organism into the peritoneal cavity through the fallopian tubes. The clinical manifestations of tuberculous peritonitis are of two types. The moist form consists of fever, ascites, abdominal pain, and weakness. The dry form presents in a similar manner but without ascites.
Answer: ABCD
DISCUSSION: Normally, there is a balance between fluid secretion and absorption in the peritoneal cavity. Ascites occurs when either the secretion rate increases or the absorption rate decreases disproportionately. Accumulation of lymph in the peritoneal cavity usually results from trauma or tumor involving lymphatic structures. Proposed treatment regimens range from salt restriction and diuretics to surgical ligation and peritoneovenous shunting. Uninfected bile is a mild irritant to the peritoneal cavity and causes increased production of peritoneal fluid, resulting in bile ascities or choleperitoneum. Most cases of choleperitoneum follow biliary tract surgery, but cases of spontaneous bile duct perforation have been reported in infants and some adults. The most common cause of hemoperitoneum is trauma to the liver or spleen. Less common causes include ruptured ectopic pregnancy, ruptured aortic aneurysms, and other intra-abdominal injuries.
Answer: b
The approach to bilateral groin hernias is based on the extent of the hernia defect. For hernias for which inguinal floor reconstruction is required (all direct and moderate to large indirect inguinal hernias, all femoral hernias), simultaneous repair of bilateral hernia results in recurrence of one or both of the hernias twice as frequently as if the hernias were repaired sequentially. Repair of recurrent inguinal or much less commonly femoral hernias can be repaired via an anterior approach particularly at the time of first recurrence in most cases. If a deficit of aponeurotic tissue exists, methods such as polypropylene mesh as an overlay or preferably as an underlay, and tailored around the spermatic cord have proved highly successful. The preperitoneal approach also has potential benefits especially in cases of multiple recurrence where the technique allows avoidance of the inevitable scar encountered with the anterior approach, excellent assessment of the defect, and the ease for placement of synthetic mesh. The Bassini and Shouldice repairs involve approximation of the medial tissues of the transversus abdominis aponeurosis and transversalis fascia to the inguinal ligament. These techniques cannot be used to repair a femoral hernia because the femoral canal lies deep to the inguinal ligament. Either the anterior approach of McVay (Cooper’s ligament repair) or a preperitoneal approach is preferred for femoral hernias. In patients with bowel obstruction attributed to a hernia, the primary operative approach is on the hernia. Assessment of bowel viability is possible without laparotomy in most cases, and release of adhesions holding the bowel within the sac is more easily accomplished through direct entry into the hernia sac. Reduction of the herniated and incarcerated bowel may be difficult from the intraabdominal approach necessitating a counter incision over the external presentation of the hernia.
Answer: a, b, c, d
Repair of an incisional hernia can be difficult with several factors making these hernias particularly challenging. First, incisional hernias are often related to a postoperative wound infection, in which case associated fascitis or muscle necrosis may result in loss of tissue. Second, a previous abdominal wall closure under tension or with a technique that resulted in tension on particular sutures may lead to a multifenestrated region of the musculoaponeurotic abdominal wall near or slightly back from its margin. Third, chronic retraction of the abdominal wall muscles result in a larger defect. Fourth, a large potential space remains anterior to the abdominal wall closure in the subcutaneous area; postoperative fluid accumulation in this space contributes to the wound infection rate of 5%. Any such potential space should have operatively placed drains.
The key to successful repair involves sufficient dissection and exposure of the true musculoaponeurotic edge and exclusion of adjacent musculoaponeurotic defects and avoidance of closing the wound under tension. Large defects greater than 3 to 4 cm in diameter are seldom able to be closed without excessive tension. The use of relaxing incisions decreases tension and may be particularly useful in midline hernias and therefore may avoid the need for prosthetic mesh.
Answer: a, b, c
The external oblique muscle and its aponeurosis, with its inferiorly and medially-directed fascicles and the overlying innominate fascia lie deep to the subcutaneous tissue. The inguinal ligament (Poupart’s ligament) is the inferior edge of the external oblique aponeurosis and extends from the anterior superior iliac spine to the pubic tubercle, turning under itself posteriorly and then superiorly to form a shelving edge. Medially, the inguinal ligament turns under even further to form the lacunar ligament, as part of its insertion on the pubis. The superficial inguinal ring is a triangular opening in the external aponeurosis, with its apex superiorly in position slightly above and lateral to the pubic tubercle, through which the cord exits the inguinal canal. The conjoined tendon is commonly alluded to in descriptions of inguinal hernia repairs. The conjoined tendon is the fusion of the aponeurosis of the internal oblique and transversus abdominis muscles.
Answer: a, b, c
The history and physical examination are almost exclusively the diagnostic modalities used for diagnosis and delineation of hernias. Chronic trauma in the form of overstretching of musculoaponeurotic structures is likely to be the significant factor in spontaneously occurring hernias. Failure to recognize underlying pathology contributing to symptoms of abdominal straining may both increase the risk of recurrent hernia as well as miss significant existing pathology. A chronic cough from chronic obstructive pulmonary disease should be investigated and attempts made to control symptoms. Significant obstructive uropathy may warrant urologic consultation and treatment prior to hernia repair. Such treatment is important both to prevent postoperative urinary retention, as well as persistent straining on the newly-completed repair. Change in bowel habits with constipation or the presence of blood associated with bowel movements may suggest a rectal or left-sided colon cancer. Patients frequently relate a specific episode of muscular straining during which a sudden discomfort occurs followed by hernia symptoms of discomfort or a bulge. There is little evidence to suggest that such a specific acute event can precipitate a hernia. A history of heavy lifting is important, however, in both planning of postoperative disability as well as consideration for long-term recurrence rates.
Answer: b, c
Hernia incarceration denotes the condition wherein viscera are contained within a hernia sac and cannot be disgorged from the sac. Patients with an incarcerated hernia may be asymptomatic except for the presence of a bulge. Pain associated with an incarcerated hernia should be interpreted as indicative of strangulation. Many hernias are of such size that they cannot be reduced either spontaneously or manually. If the patient is asymptomatic, elective surgery should be planned. In a patient with pain, attempt at reduction is relatively safe as long as excessive force is not applied. An incarcerated hernia with discomfort or signs of bowel obstruction is best treated with urgent hernia repair, although gentle attempts at reduction may be without consequences. Reduction of a symptomatic hernia may result in reduction of gangrenous bowel into the peritoneal cavity. Reduction of bowel with necrotic areas eventuates in bowel perforation and peritonitis with an associated 10% to 30% mortality and high levels of morbidity. Vigorous attempts at reduction may result in reduction en masse, in which the viscera remain within the peritoneal sac after reduction with the entire sac and its contained viscera forced through the abdominal wall defect into the preperitoneal layer. Reduction en masse usually occurs when a small fibrous neck traps enclosed viscera and is associated with a high risk of continued entrapment and progression to obstruction or strangulation.
World-wide hernias are the leading cause of intestinal obstruction. The obstruction is almost exclusively small intestinal with only rarely the colon as the site of obstruction.
Answer: a, b, c
Ninety percent of patients with retroperitoneal fibrosis present with dull, non-colicky pain in the back, flank, or abdomen. Other symptoms include weight loss, non-specific gastrointestinal complaints, and uncommonly, lower extremity edema, malaise, and dysuria. Laboratory studies may be normal in 25% of patients, but 55% of patients will have an elevated blood urea nitrogen. Diagnosis is most commonly suggested by intravenous pyelography. The combination of medial deviation of the ureter, hydroureteronephrosis, and extrinsic ureteral compression are highly suggestive of retroperitoneal fibrosis. CT scanning or MRI can both define the level of ureteral involvement and depict the mass appearance of the fibrotic process. Exploratory laparotomy with multiple deep biopsies of the retroperitoneal process is an essential part of diagnosis, since foci of carcinoma may be sparse within the predominately sclerotic reaction.
Treatment for retroperitoneal fibrosis must identify and deal with potential causative agents, relieve the ureteral obstruction, and reverse the inflammatory-fibrotic process. Renal obstruction may need to be relieved acutely, either by retrograde ureteral stents or by percutaneous nephrostomy tubes. Long-term resolution of ureteral obstruction most frequently has been accomplished by operative freeing of the ureters from the fibrosis and displacing them laterally or within the peritoneal cavity. Although renal function is improved in more than 90% of cases so treated, in as many as one-third of patients, ureteral obstruction recurs on the ipsilateral or contralateral side. Prognosis for patients with nonmalignant retroperitoneal fibrosis is good. Survivals of 86–100% for several years have been reported.
Answer: b, c
Rectus sheath hematoma results from arterial or venous bleeding into the rectus sheath, most commonly from arterial bleeding. Rectus sheath hematomas predominate in women by a ratio of about 3:1. The mean age of incidence is in the late fifth decade. Although spontaneous formation of a rectus hematoma is rare, it can occur with vasculitis, arterial venous malformations, a severe coagulopathy, or with the administration of anticoagulants. The usual cause is trauma. Events as trivial as sneezing, coughing, or twisting to the side have initiated a rectus hematoma. Abdominal pain is almost always described at presentation. Pain is often described as severe and usually is exacerbated by movements that require muscular contraction of the abdominal wall. On examination, there is tenderness over the rectus sheath, voluntary guarding, and often a diffuse mass sensation in the area of tenderness. Contraction of the rectus muscle exacerbates the pain and tenderness. Peritoneal signs are absent. Ecchymosis may occur but usually appears several days after the onset of pain. In cases where the hematoma dissects or originates inferiorly and expands into the prevessicle and preperitoneal space, the hematocrit may fall significantly; however, hemodynamic instability is distinctly unusual. When the intraabdominal source of pain is unknown, ultrasound and particularly computed tomography can delineate the hematoma and localize it to the abdominal wall in almost all cases.
Treatment must take into consideration the cause, if known, and whether the hematoma is stable or progressive. Coagulopathy should be corrected when possible. For patients in whom the hematoma is stable, pain medication and avoidance of muscular stress on the abdominal wall are sufficient. For patients with progressive hematoma, the treatment of choice is evacuation of the hematoma from within the rectus sheath and hemostasis, sometimes requiring ligation of the epigastric vessels above and below the hematoma.
Answer: b, c
The anterior abdominal wall consists of a group of lateral sheet-like muscles and paired, longitudinally-oriented flat muscles on either side of the midline. The lateral musculature of the abdominal wall consists of three layers, each of which has its fascicles running in an oblique angle to the others. The most superficial of these lateral muscles is the external oblique muscle. The internal oblique muscle lies deep to the external oblique muscle while the transversus abdominis muscle is the innermost of the lateral abdominal wall musculature. The transversalis fascia lies on the deep side of the transversus muscle and extends to form an essentially complete fascial envelope of the abdominal cavity. The semicircular line is defined by the lower edge of the posterior sheath about 3 to 6 cm below the level of the umbilicus, and its convexity is directed superiorly. Above the semicircular line, the internal oblique aponeurosis splits into posterior and anterior laminae. The posterior lamina joins with the transversus abdominis aponeurosis to form the posterior rectus sheath. The anterior lamina fuses with the external oblique aponeurosis to form the anterior rectus sheath. Below the semicircular line, the internal oblique end transversus abdominis aponeurosis fuse to form an internal lamina of the anterior sheath, with the external oblique aponeurosis forming the external lamina of the anterior sheath. The medial paired rectus abdominis muscles originate on the ribs superiorly and on the pubis inferiorly. Below the semicircular line, the rectus muscles are nearly fused in the midline and indistinct, and their posterior surfaces covered only with the transversalis fascia.
The Correct Answer is a
The structure of secretin is different from that of CCK and gastrin but very similar to that of glucagon, GLI, VIP, and GIP.
William F. Ganong - 2005
Answer: a, b
Retroperitoneal fibrosis is a rare condition in which fibrosis develops in the retroperitoneal space. The ureters frequently will become encompassed by the process eventually causing hydronephrosis and kidney damage. Retroperitoneal fibrosis occurs most commonly in the fifth and sixth decades with a 2:1 male-female predominance. The pathophysiology of retroperitoneal fibrosis remains to be delineated. In fully two-thirds of cases, retroperitoneal fibrosis is idiopathic, however, an autoimmune process has been suggested as a potential cause. About 12% of cases of retroperitoneal fibrosis have been associated with the use of methysergide, a serotonin agonist used for vascular and migraine headache, and in this subgroup females outnumber males 2:1.
Primary or metastatic malignancy in the retroperitoneum is found in 8% of patients with retroperitoneal fibrosis. Sarcomas are the most common primary tumors, but non-Hodgkin and Hodgkin lymphomas and ureteral cancer have also been found.
Metastases have originated from cancer of the stomach, breast, colon, carcinoid, pancreas, prostate, ovary, and cervix. The focus of tumor may be small but may induce desmoplasia that is grossly indistinguishable from benign variance of retroperitoneal fibrosis.
Answer: b
An umbilical hernia in a child is usually considered to be congenital. Only about 10% of umbilical hernias in adults are thought to be the result of a congenital defect carried into adulthood. Most adult umbilical hernias are acquired and are called paraumbilical hernias. The paraumbilical hernia typically occurs in a multiparous female. Other patients with increased intraabdominal pressure, particularly with concomitant chronic abdominal distension as from ascites, are also at increased risk for the development of paraumbilical hernias. Umbilical and paraumbilical hernias vary from small to extremely large. Incarceration is frequent in the large hernias, which typically have a small neck.
Indications for umbilical hernia repair in adults include symptoms, incarceration, large hernia relative to the neck, and trophic changes in the overlying skin. Among adults with associated ascites, repair is advocated to avoid potentially serious complications. The presence of discoloration or ulceration of overlying skin or a rapid increase in size of the hernia herald impending rupture. Spontaneous rupture of the hernia in these patients can be catastrophic and is frequently associated with mortality rates approaching 30%. By comparison, elective umbilical hernia repair can be performed safely in patients with ascites with acceptable morbidity and mortality.
Answer: c
An obturator hernia is a hernia that occurs through the obturator canal, accompanied by the obturator vessels and the obturator nerve. Although rare, most obturator hernias occur in older multiparous women and are predominantly right-sided.
Symptoms are frequently intermittent but tend to be acute and become increasingly severe with incarceration of the hernia. Intestinal symptoms predominate, but dysesthesia or pain in the medial thigh with occasional radiation to the hip is often present. Dysesthesia results from compression of either division of the obturator nerve. Although the hernia is never externally visible, in a small percentage of patients a mass can be palpated in the upper, medial thigh. A correct diagnosis of obturator hernia is made in only about one-third of patients presenting with intestinal obstruction. Plain radiographs are seldom helpful, however a CT scan will usually confirm the diagnosis. Treatment is operative. There is no place for expectant therapy, especially in a patient with pain an parasthesias along the inner aspect of the thigh or with clinical or radiographic evidence of bowel obstruction.
Many surgical approaches have been promoted, but the transabdominal approach should be used because it has several advantages. It best confirms the diagnosis and exposes the obturator canal, orifice, vessels, and nerve, also permitting bowel resection when required. The sac is dealt with in a standard fashion. The hernia defect should be repaired, but repair usually requires a polypropylene mesh patch because the margin of the defect cannot be approximated primarily.
Answer: a, c
Inguinal hernias are the most frequently occurring hernia by a factor of five over other individual types. Umbilical hernias constitute about 14% of hernias, femoral hernias about 5%, and other types are rare. There is a male prevalence in inguinal hernias of about 7:1 (male-to-female), whereas there is a female dominance in femoral and umbilical hernias of 8:1 and 7:1 (female-to-male), respectively. For inguinal hernia, which occurs at all age levels, frequency increases with age. Umbilical hernias have a bimodal distribution, peaking in the pediatric population and then in the 40 to 60 year group, in which the hernias are principally paraumbilical.
Answer: a, c, d
The Bassini repair is an inguinal hernia repair used world-wide and has been the standard against which other repairs are judged. The repair involves approximation of the transversus abdominis aponeurosis and transversalis fascia and the lateral edge of the rectus sheath to the shelving edge of the inguinal ligament. A femoral hernia cannot be repaired by the Bassini repair because the orifice to the femoral canal lies deep to the inguinal ligament. A Cooper’s ligament repair does approximate the structures to the transversalis fascia of the pectineal (Cooper’s) ligament between the pubic tubercle and the femoral vein and therefore is appropriate for repair of a femoral hernia.
A relaxing incision for repairs of direct and large indirect inguinal hernias prevents excessive tension in the closure. There are an increasing number of proponents for the use of prosthetic material for the routine repair of inguinal hernias. Prosthetic material, such as polypropylene mesh, have been used for years for repair of large or recurrent inguinal and femoral hernias. The prosthetic mesh provides a low-tension repair for such large defects which otherwise could not be closed without excessive tension. In addition, the mesh incites the formation of scar tissue to further increase tensile strength beyond that provided by mesh alone.
Results reported for inguinal hernia repairs using mesh have been excellent, although there is a slight risk of infection of the prosthetic material which must be considered.
Answer: a
Desmoid tumors are fibromatous tumors that may resemble low-grade fibrosarcoma but never metastasize. The tumor often infiltrates adjacent muscle and has a high incidence of recurrence despite seemingly adequate gross resection. The highest frequency is in women of childbearing age of which over 90% of tumors are abdominal in location. For abdominal wall desmoid tumors, approximately one-third are associated with a previous operation at the tumor site. The most frequent presenting symptom is a nontender, palpable abdominal wall mass.
Diagnostic imaging is best carried out by CT or MRI, which delineate the extent of involvement of the layers of the abdominal wall and potential intraperitoneal extension. Initial treatment of abdominal wall desmoid tumors is surgical. Because the margins of the tumor are not easily determined and because the tumor often infiltrates muscle and periosteum, limited margins around the gross tumor frequently result in microscopic tumor at the margin. Recurrence rates for abdominal desmoid tumors vary from 9% to 40%, and recurrence is frequent with inadequate margins. A 5-cm margin of resection is considered adequate with mono bloc resection of rib cage, pubic or iliac bone or involved portions of organs such as bladder to achieve these margins.
Reconstruction of the abdominal wall with polypropylene mesh is necessary in most cases. In patients in whom adequate margins of resection are achieved, there is no benefit from adjuvant radiotherapy. Second and third resections after recurrence have been associated with no higher rate of recurrence than primary resection.
Radiotherapy alone has achieved local control in desmoid tumor in as many as 100% of tumors treated primarily and 75% of recurrent tumors. Radiation doses at least 60 Gy are considered necessary for consistent control. The large radiation dose risks major damage to adjacent bowel and therefore primary radiation treatment of abdominal wall desmoid tumors has a limited role.
Answer: a, b, c
The laparoscopic approach to the repair of groin hernias has been recently developed. Either a transabdominal approach, wherein the peritoneum in the inguinal area is opened, and the repair is performed in the preperitoneum or an entirely preperitoneal approach can be used. In either technique, which are both performed under general anesthesia, after reducing the visceral contents out of the hernia, the repair is performed by placing a sheet of prosthetic mesh over the internal aspect of the inguinal floor and internal ring. Although early results and short-term benefits appear promising, long-term follow-up data is still not available to compare these techniques with traditional repairs.
Answer: a, b, e
Chylous ascites is accumulation within the peritoneal cavity of chyle, a lymphatic fluid with a high lipid content. Access of intestinal lipids to the circulation is via mesenteric lymphatics that enter the cisterna chyle, which in turn becomes the thoracic duct which eventually enters the venous system at the junction of the left subclavian and internal jugular veins. The cisterna chyli lies at the anterior surface of the first and second lumbar vertebrae slightly to the right of the aorta. Chylous ascites may result from injury to major lymphatic duct or the cisterna. However for lymphatic leakage to persist, widespread occlusion of lymphaticovenous collaterals within the abdomen must be present. Malignancy is the predominant cause (88%) of spontaneous chylous ascites in adults, with lymphoma the most common malignancy. Diagnostic studies must include not only documentation of lymphatic origin of the abdominal fluid but also an attempt to delineate the cause of chylous ascites. Paracentesis and analysis of chylous fluid typically reveals elevated triglycerides, protein, and leukocyte levels, with a predominance of lymphocytes. Unfortunately, cytology is seldom positive despite the presence of malignancy. Lymphangiography may define the site of lymphatic leak for patients in whom the leak is from the cisterna or retroperitoneal lymphatics but not when from the mesenteric or hepatic lymphatics. Of noninvasive studies, CT is the test of choice, with a high diagnostic yield in nontraumatic chylous ascites in adults. Frequently, laparotomy with node biopsy is required for histology and typing in cases suspected to be cancer, particularly for lymphoma.
Treatments for chylous ascites have been directed toward decreasing lymph and triglyceride accumulation.
Successful resolution of chylous ascites has been achieved using a fat-restricted diet with added medium-chain triglycerides in an attempt to reduce lymphatic transport of triglycerides and perhaps intestinal lymph flow. Although there have been reports of success using such dietary manipulation, many failures have been reported. Therefore, in most patients with chylous ascites, treatment is likely to be successful only when directed toward the underlying cause. For patients with lymphoma, therapy effective against lymphoma is likely to eliminate chylous ascites.
The prognosis for patients with chylous ascites is much better in infants and children than in adults, principally because of the differences in causes of the condition. A mortality of 21% is reported in infants and children whereas a mortality of 88% has been noted in adults. Patients with chylous ascites with associated neoplasms typically have the gravest prognosis.
Answer: a, c, d
Many complications can occur with operations to repair an inguinal hernia. Sensory nerve injury may lead to disabling symptoms from neuromas or nerve entrapment during inguinal hernia repair. Although vascular injuries are uncommon in inguinal repair, the proximity of the femoral vein to the structures used in the hernia repair makes injury of this vessel the most frequent vascular injury observed. Hernia recurrence after primary groin hernia repairs should be infrequent and varies in several large series from less than one percent to almost nine percent. The prevalence of recurrent hernia may be higher after repair of recurrent groin hernia. Factors responsible for hernia recurrence include closure under excessive tension, failure to identify and use an adequately strong musculoaponeurotic tissue, and wound infection.
Answer: b, c
Arising anteriorly from the external iliac artery, the inferior epigastric artery with its accompanying vein runs obliquely medially and upward in the preperitoneal fat, posterior to the transversalis fascia and close to the inferior margin of the internal inguinal ring. Inguinal hernias arising superior to the inferior epigastric vessels are indirect inguinal hernias, whereas those arising inferior to the vessels are direct inguinal hernias. The iliohypogastric and ilioinguinal nerves are motor and sensory nerves to the muscles and skin of the inguinal region. The nerves penetrate the transversus abdominis muscle at the point above the middle of the iliac crest, lie below the internal oblique muscle up to the point just medial and superior to the anterior superior iliac spine, and then penetrate the internal oblique muscle and lie below the external oblique aponeurosis. The ilioinguinal nerve runs anterior to the spermatic cord in the inguinal canal and at the superficial inguinal ligament, branches into sensory supply to the pubic region and the upper scrotum or labium majoris. The genital branch of the genitofemoral nerve perforates the transversalis fascia usually just inferior to the internal ring. It courses along the posterior surface of the spermatic cord and supplies motor fibers to the cremaster muscle. At the superficial inguinal ring, it divides to provide sensory innervation to the scrotum and medial aspect of the upper thigh.
 Answer: A
Answer: A

 Answer: C
Answer: C
Answer: C

Answer: ACDE

DISCUSSION: The columnar epithelial cells are responsible for absorption. These cells exhibit a striated luminal border or brush border. The microvilli account for the appearance of the brush border. The microvilli greatly increase the absorption surface of the epithelial cell. The brush border contains disaccharidase in high concentrations. In addition to increasing surface area the microvilli perform an important digestive function.
Answer: ACEF
DISCUSSION: The mucosa of the small intestine encompasses the epithelium, the lamina propria, and the muscularis mucosae. The lamina propria between the epithelium and the muscularis mucosae contains blood and lymph vessels, nerve fibers, smooth muscle fibers, fibroblasts, macrophages, plasma cells, lymphocytes, eosinophils, and mast cells, as well as connective tissue elements.
Answer: ACEF
DISCUSSION: Amylopectin, the most abundant constituent of starch, is a 1-4–linked straight chain of glucose molecules. In addition, amylopectin possesses a 1-6 branching side chain at approximately every 25 glucose units along the straight chain. Amylase has only 1-4 linkages of glucose molecules. Pancreatic and salivary amylase break the interior 1-4 glucose linkages.

Answer: ABCDE

DISCUSSION: One of the most important events during simple mechanical small bowel obstruction, loss of water and electrolytes from the body, is caused mainly by intestinal distention. Distention may produce reflex vomiting. Distention causes intestinal secretion. Distention causes decreased absorption.


Answer: ADE
DISCUSSION: Micellar solution provides an optimal environment for the action of pancreatic lipase. Pro-co-lipase is converted to co-lipase by trypsin. Co-lipase binds to triglyceride, then lipase complexes with co-lipase, and triglyceride hydrolysis access. Pancreatic lipase hydrolyzes triglyceride into 2-monoglyceride and fatty acids. The 2-monoglyceride and fatty acid enter the micellae. An alkaline pH allows lipase to function optimally. Micellar fatty acids and 2-monoglyceride pass into the epithelial cell by diffusion.
Answer: AB
DISCUSSION: Abdominal x-ray examination of patients with intestinal obstruction usually reveals abnormally large quantities of gas in the bowel. One can usually identify distended small intestine or colon. Gas in the small bowel outlines the valvulae conniventes, which usually occupy the entire transverse diameter of the bowel image. Colonic haustral markings occupy only a portion of the transverse diameter of the bowel.
Typically, the small bowel pattern occupies the more central portion of the abdomen, whereas the colon shadow is on the periphery of the abdominal files or in the pelvis. Patients with mechanical small intestinal obstruction usually have minimal colonic gas, if any.


Answer: ABCDF
DISCUSSION: History and physical examination permit the diagnosis of intestinal obstruction. Any patient having crampy abdominal pain, vomiting, obstipation, abdominal distention, abdominal tenderness, and peristaltic rushes should be managed for intestinal obstruction until the diagnosis can confidently be excluded.


Answer: C
DISCUSSION: Meckel's diverticulum is a true diverticulum containing all layers of the intestinal wall, usually arising from the antimesenteric border of the ileum 45–90 cm. proximal to the ileocecal valve. It is a vestige of the omphalomesenteric or vitelline duct, which usually undergoes complete obliteration during the seventh week of gestation. Autopsy studies have estimated the incidence of Meckel's diverticulum to be 1% to 2% with men being more commonly affected than women by a ratio of 2:1. Gastric mucosa is present in 50% of all Meckel's diverticula, but in over 75% of symptomatic individuals.
Answer: A
DISCUSSION: It is estimated that only 4% of patients who possess a Meckel's diverticulum will become
symptomatic during their lifetimes.
The most common clinical presentation is incidental identification during abdominal exploration. Symptomatic presentations are secondary to hemorrhage, small bowel obstruction, diverticulitis, perforation, associated umbilical abnormalities, and tumors. Over half of patients presenting with symptoms are under the age of 2.
The most common clinical problem associated with Meckel's diverticulum is gastrointestinal bleeding presenting as bright red blood per rectum. The usual source of the bleeding is a chronic acid-induced ileal ulcer in the ileum adjacent to a Meckel's diverticulum that contains gastric mucosa. Another common symptom associated with a Meckel's diverticulum is intestinal obstruction.
The cause of this obstruction may be volvulus of the small bowel around a diverticulum associated with a fibrotic band attached to the abdominal wall, intussusception, or rarely, incarceration of the diverticulum in an inguinal hernia (Littre's hernia).
Volvulus is usually an acute event and if allowed to progress, may result in strangulation of the involved bowel. In intussusception, a broad-based diverticulum invaginates and then is carried forward by peristalsis.
Answer: ABD
DISCUSSION: Carcinoid tumors should be treated by resection, regardless of the presence of metastases, because growth of the primary neoplasm is slow and local complications, such as obstruction and intussusception, are frequent. At clinical discovery a large percentage (as many as 70%) of small-intestinal carcinoids are metastatic to lymph nodes and/or liver. All tumors should be managed by wide en bloc resection, regardless of the size of the primary lesion or the presence of distant metastases. Lesions in the distal ileum require ileocolectomy. Appendiceal tumors larger than 1.5 cm. should be treated by ileocolectomy. The incidence of metastases depends on the size and location of the primary tumor. Appendiceal carcinoid tumors smaller than 1.5 cm. are rarely malignant and may be treated safely by routine appendectomy. This is not true of larger tumors. Like carcinoid tumors elsewhere in the gastrointestinal tract, the malignancy potential of rectal carcinoid tumors is directly proportional to their size. Tumors smaller than 1 cm. have little or no malignant potential and may be treated by endoscopic excision. Tumors measuring 1 to 2 cm. should be excised operatively with margins, but when they are larger than 2 cm. rectal carcinoid tumors may require anterior resection. In patients with ileal carcinoid tumors, the evidence of a second tumor has been reported as high as 40%. Thus, the search for synchronous metachronous and metastatic neoplasms should be undertaken.
Answer: CD
DISCUSSION: Carcinoid syndrome occurs when venous drainage from the tumor gains access to the systemic circulation, escaping hepatic degradation. Although hepatic metastases are most often responsible, retroperitoneal metastases and bronchial, ovarian, and testicular carcinoid tumors can also cause the carcinoid syndrome. Serotonin is thought to be largely responsible for both the diarrhea and the fibrosing cardiac lesions associated with the carcinoid syndrome. The vasomotor changes, however, are mediated by kinins and such vasoactive peptides as substance P, neuropeptide K, neurokinin A, and neurotensin. Other substances, such as histamine, vasoactive intestinal peptide (VIP), and prostaglandins, may also contribute to systemic manifestations in the carcinoid syndrome. Foregut carcinoid tumors, of which stomach and bronchial tumors are the most common, can cause atypical carcinoid syndrome. It is thought that these tumors are deficient in the enzyme dopa-decarboxylase and have impaired conversion of 5-hydroxytryptophan (5-HTP) into 5-hydroxytryptamine (5-HT), leading to secretion of 5-HTP into the vascular compartment. Some of the 5-HTP is converted into 5-HT and 5-hydroxyindoleacetic acid (5-HIAA) in extrarenal sites, and some is decarboxylated in the kidney and excreted into the urine as 5-HT; but some of the 5-HTP is excreted directly into the urine. Thus, in patients with foregut tumors, the urine contains relatively little 5-HIAA (but more than normal) but large amounts of 5-HTP and 5-HT, in contrast to patients with midgut carcinoid tumors in which large amounts of 5-HIAA are secreted into the urine but relatively little 5-HTP. Carcinoid tumors of the hindgut contain no argentaffin or argyrophil cells, they have no secretory products, and therefore they are not associated with the carcinoid syndrome. The long-acting somatostatin analog provides the best symptomatic therapy, because somatostatin inhibits both release and action of humoral mediators of the carcinoid syndrome. By contrast, serotonin antagonists are of little value and the efficacy of interferon therapy has yet to be established.
Answer: ABD
DISCUSSION: The 72-hour stool collection is quite sensitive and detects even mild malabsorption. As it requires careful stool collection timed by carmen red markers and documented dietary fat intake, it is not useful for screening. Microscopic examination of the stool can detect muscle fibers if protein malabsorption is present and with Sudan II staining can estimate fat content. D-Xylose absorption from oral ingestion of 5 gm., detected by a blood sample after 1 hour, is a simple and quite accurate test to identify carbohydrate malabsorption. Small bowel x-ray series, using barium contrast, can give very useful information on mucosal abnormalities, enteric fistulas, mechanical obstructions, and very importantly, intestinal motility and transit time.
Answer: ABD
DISCUSSION: Once the stress of the surgical procedure is over, there is no further hypermetabolic response, nor does there appear to be any reduced energy expenditure from loss of the metabolically active small bowel. Energy needs are unaltered. Gastric secretion and hyperacidity are directly related to the extent of small bowel resection and is due in part to increased concentrations of gastrin in the serum. H 2 blockers are effective in reducing acidity and volume of gastric secretions. Hyperoxaluria develops owing to binding of calcium to fat in the diet with steatorrhea, leaving less to bind with dietary oxalate. The soluble oxalate is absorbed by the colon and excreted in the urine. If oxalate is excessive, oxalate kidney stones can form. With fat malabsorption due to bile salt depletion and rapid intestinal transit, absorption of the fat-soluble vitamins A, E, K, and D is reduced. Even with oral supplementation, deficiencies can develop.
Answer: E
DISCUSSION: These physical factors are interactive. Less energy is delivered through a small portal than through a large one. Multiple portals permit concentration of the radiation in the area to be treated and spare skin and viscera from damage. There is less risk of injury from irradiation of a given intensity if more fractions are applied.
Answer: B
DISCUSSION: Patients who have symptoms of vascular compromise or evidence of perforation require urgent laparotomy. Patients with small bowel obstruction may require a laparotomy if a complete obstruction persists, but gastrointestinal decompression and hydration are first steps. Patients with radiation-induced rectovaginal fistula may require temporary or even permanent colostomy, but the first steps are evaluation and control of sepsis. Malabsorption and diarrhea can generally be controlled pharmacologically. Rectal stenosis can usually be managed without laparotomy.
Answer: b
Gut-associated lymphoid tissue (GALT) represent a major division of the immune system and is made up of aggregated (Peyer’s patches, lymphoid follicles, mesenteric lymph nodes) and nonaggregated cellular components. The lamina propria of the small intestine contains a wide array of nonaggregated lymphoid tissue including B cells, T cells, macrophages, eosinophils, and mast cells. Some 80% to 99% of B cells are active producers of immunoglobulin A (IgA). In comparison, only 2% to 5% of B cells found in other lymphoid tissues of the body secrete IgA. IgA is the major immunoglobulin of the intestinal immune system. The functional characteristics of IgA are unlike those of other antibodies. Unlike IgG or IgM, secretory IgA does not induce Fc-mediated inflammatory reactions. Antigen-IgA complexes do not activate the classic or alternate complement systems, nor does IgA promote the phagocytosis of bacteria by opsonization. Most of the protective effect of IgA derives from its ability to bind the threatening antigen efficiently, while resisting enzymatic degradation by gut enzymes.
Answer: a, d
The migrating motor complex (MMC) is a cyclic pattern of spike bursts and muscular contractions that migrate from the duodenum to the terminal ileum. The MMC is divided into four phases: phase I-the period of quiescence with no activity; phase II-accelerating irregular spike activity; phase III-the activity front with a series of high-amplitude, rapid spikes corresponding to strong, rhythmic gut contractions; and phase IV-subsiding activity. In humans the cycle lasts about 90 to 120 minutes. Each phase passes in sequence along the bowel, and when the terminal ileum is reached, the process resumes in the proximal gut. This interdigestive cycle is interrupted and replaced by rapid spiking activity (similar to phase II) when the gut receives a food bolus. The duration of the interruption depends on the volume and nature of the food stuffs with fats causing the largest duration of rapid spiking. Blood levels of the GI hormone, motilin, correlate closely with MMC activity and exogenous motilin can induce the MMC front. Other hormones whose serum levels parallel MMC activity are pancreatic polypeptide and somatostatin. Drugs that can initiate the MMC front include histamine, metoclopramide, and morphine.
Answer: a, b
The duodenum is divided into four parts-the bulb, followed by the second (descending), third (transverse), and fourth (ascending) portion. The duodenal bulb begins at the pylorus and extends for the next 5 cm as the duodenum assumes a retroperitoneal position for the second, third, and fourth portion. The third and fourth portion of the duodenum complete the duodenal sweep. Mobilization of the duodenum from the retroperitoneum for a multitude of abdominal procedures can be facilitated by the Kocher maneuver where the retroperitoneal attachment is divided and the duodenum and head of the pancreas can be brought out of its retroperitoneal position. Endoscopically, the major papilla of the duodenum can be seen entering at the mid-point of the second portion of the duodenum. The papilla (ampulla of Vater) appears anatomically as a hooded fold, marking the confluence of the common bile duct and the main pancreatic duct (duct of Wirsung) and is surrounded by the muscular sphincter of Oddi. In some 50% to 60% of patients, an accessory pancreatic duct (the duct of Santorini) can be seen entering the duodenum proximal to the ampulla of Vater. Endoscopically, this lesser, or minor, papilla appears as a one-to-three mm sessile polyp. The jejunum is the portion of the small bowel that courses from the ligament of Treitz to an arbitrary point approximately two-fifths of the distance to the ileocecal valve. The length of the jejunum has been estimated at 100 cm although this distance can vary dramatically depending on the status of the small intestine. The jejunum is the widest portion of the small intestine, and the diameter progressively decreases as the ileocecal valve is approached. The ileum makes up the distal three-fifths of the combined jejunal/ileal length.
The Correct Answer is B
Neurotransmitters bind with receptors that also act as ion channels or they interact with G-proteins to stimulate effector enzymes to produce “second messengers”.
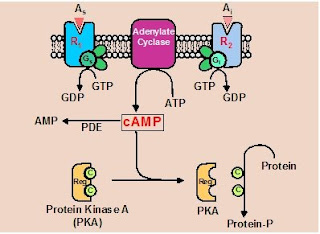
Figure 3. cAMP as a second messanger. cAMP is made from ATP by the enzyme adenylate yclase. CAMP is broken down by phosphodiesterase (PDE). The activity of adenylate cyclase can be modulated in by G-proteins. When stimulatory agonixts (As)bind with their receptors the stimulate G-proteins of the Gs class. This increases adenylate cyclase activity and cAMP levels. When inhibitory agonixts (Ai)bind with their receptors the stimulate G-proteins of the Gi class. This decreases adenylate cyclase activity and cAMP levels. cAMP exerts its effect by activating protein kinase A (PKA) which phosphorylate proteins, e.g. enzymes and pumps, and in turn increases or decreases their activity.
Phospholipase C, diacylglycerol and inositol trisphosphate - The relevant G protein (termed Gq), activated by a first-messenger-bound receptor, activates a plasma-membrane effector enzyme called phospholipase C.
- This enzyme catalyzes the breakdown of a plasma-membrane phospholipid known as phosphatidylinositol bisphosphate, abbreviated PIP2, to diacylglycerol (DAG) and inositol trisphosphate (IP3).
- Both DAG and IP3 then function as second messengers but in very different ways.
- DAG activates a particular protein kinase known as protein kinase C, which then phosphorylates a large number of other proteins, leading to the cell's response.
- IP3, does not exert its second messenger role by directly activating a protein kinase.
- IP3, after entering the cytosol, binds to calcium channels on the outer membranes of the endoplasmic reticulum and opens them.
- Because the concentration of calcium is much higher in the endoplasmic reticulum than in the cytosol, calcium diffuses out of this organelle into the cytosol
- Increases cytosolic calcium concentration.
- This increased calcium concentration then continues the sequence of events leading to the cell's response to the first messenger
Answer: a, c
The endocrine functions of the small intestine are diverse with an ever increasing number of hormones, peptides, neurotransmitters, and paracrine substances identified. Cholecystokinin (CCK) is produced by cells located primarily in the mucosa of the duodenum and jejunum and released in response to luminal fats and proteins. After CCK release from the duodenum and jejunum, the gallbladder contracts and the sphincter of Oddi relaxes, emptying bile into the duodenum. Secretin is found in the S cells of the duodenum and jejunum. Secretin, a true hormone, is released in response to acid in the duodenum when luminal pH falls below 4.5. Intraduodenal secretion of pancreatic bicarbonate neutralizes duodenal pH and results in diminished release of secretin. CCK acts in a synergistic fashion with secretin to stimulate pancreatic exocrine function. Motilin is a 22-amino acid peptide localized in the enterochromaffin cells of the mucosa of the upper small intestine. Motilin likely has a physiologic role in the regulation of the migrating motor complex (MMC). Motilin is released during the fasting state, and increased levels correspond with the onset of the MMC. Neurotensin is a 13-amino acid neurotransmitter found in the central nervous system and in the gut. Specific endocrine cells that contain neurotensin are found in the ileal mucosa with smaller quantities found in the jejunum, stomach, duodenum, and colonic mucosa. Neurotensin is released by a mixed meal and fats, with carbohydrates and protein releasing much smaller increments. It has been proposed that neurotensin has a physiologic role in fat-initiated changes in gastric acid secretion, gastric emptying, pancreatic secretion, and intestinal motility.
Answer: a, c
Some 80% to 90% of bile salts secreted into the small intestine as micelles are reabsorbed and returned to the liver through the portal circulation. This circular flow of bile is termed the enterohepatic circulation. In the liver, bile salts are resecreted and stored in the gallbladder in preparation for the next meal. The reabsorption process of bile is both passive and active. Passive absorption occurs along the entire length of the small bowel and depends on the lipid solubility of the bile salt. Glycine bile conjugates are more soluble than taurine conjugates. As much as 50% of bile is passively reabsorbed. Active absorption of bile occurs only in the terminal ileum. A small amount of bile escapes into the colon, where it is deconjugated by bacteria, promoting lipid solubility and further passive absorption. High colonic concentration of bile salts promote diarrhea by inhibiting sodium and water absorption. This commonly occurs in patients with ileal resection and can be treated with the bile-binding resin, cholestyramine.
Answer: b, c, d
The jejunum is the site of maximum absorption of all ingested materials expect for vitamin B12. Although its mucosa contains numerous specific transport processes, the presence of large intercellular pores produces a permeable membrane and allows for rapid passive transfer or solutes and water. The ileum is less permeable and makes greater use of active-transport mechanisms. Normally about 1 to 1.5 liters of water is ingested each day with another 5 to 10 liters secreted by the GI tract in some form. About 80% of this fluid is absorbed by the small bowel. Because of this large bidirectional movement of water, a small alteration in bowel permeability or transport can rapidly result in net secretion and diarrheal disease states. A major source of caloric nutrition comes in the form of carbohydrate. In the Western diet, this is made up primarily of starch (about 60%), sucrose (30%), and lactose (10%). The digestive process for starch begins with digestion of the polysaccharide first by salivary amylase and continues with pancreatic amylase yielding smaller oligosaccharides which along with sucrose and lactose are then presented to the brush border of the jejunum to complete the digestion and absorptive processes. Dietary fiber consists of nondigestible carbohydrate, such as cellulose. Fiber is found commonly in all-bran cereals, beans, partially cooked vegetables, and raw pulpy fruits. High fiber diets retain water within the bowel lumen and significantly shorten bowel transit time. Dietary fiber can absorb organic materials such as bile salts and lipids and inorganic materials such as zinc, calcium, magnesium and iron.
Answer: b, c
When a loop of bowel is obstructed, intestinal gas and fluid accumulate. Approximately 80% of the gas seen on plane abdominal radiographs is attributable to swallowed air. In the setting of acute pain and anxiety, patients with intestinal obstruction may swallow excessive amounts of air. Fluid accumulates intraluminally with open-or closed-loop small intestinal obstruction due to a number of factors. Experimental studies and clinical investigations demonstrate that elevation of luminal pressures above 20 cm H2O inhibits absorption and stimulates secretion of salt and water into the lumen proximal to an obstruction. In closed-loop obstruction, luminal pressures may exceed 50 cm H2O and may account for a substantial proportion of a luminal fluid accumulation. In simple, open-loop obstruction, distention of the lumen by gas rarely leads to a luminal pressure higher than 8–12 cm H2O. Thus, in open-loop obstruction, the contributions of high luminal pressures to hypersecretion may not be important. In response to heightened luminal pressure, total blood flow to the bowel may initially increase. Subsequently, however, blood flow to the bowel is compromised as luminal pressures increase, bacteria invade, and inflammation leads to edema within the bowel wall. Accumulation of gas and fluid in the obstructed lumen also leads to changes in myoelectrical function in the gut, proximal and distal to the obstructed segment. In response to distension, the obstructed segment itself may dilate, a process known as “receptive relaxation.” At sites proximal and distal to the obstruction, changes in myoelectrical activity are time-dependent. Initially, there may be intense periods of activity and peristalsis. Subsequently, myoelectrical activity is diminished and interdigestive migrating myoelectrical complex (MMC) is replaced by ineffectual and seemingly disorganized clusters of contractions.
Answer: a, d
Peritoneal adhesions account for more than half of small bowel obstruction cases. Lower abdominal procedures such as appendectomy, hysterectomy, and abdominal perineal resection are common precursor operations to account for obstruction although adhesions may follow any abdominal procedure including cholecystectomy, gastrectomy, and abdominal vascular procedures. Simple adhesive obstruction is distinguished from other forms of obstruction by the capacity to resolve without surgical intervention. In recent surveys, as many as 80% of episodes of small bowel obstruction due to adhesions may resolve nonoperatively. The likelihood that an obstruction is due to recurrent malignancy relates to several factors including the origin of the primary malignancy, the stage of the primary malignancy, and the designation of original surgery as curative or palliative. Gastric and pancreatic cancers often present with, or are subsequently complicated by peritoneal carcinomatosis and subsequent obstruction. With respect to colon and rectal carcinomas, as many as 50% of cases presenting with obstruction after resection of the primary may be due to adhesions and not recurrent malignancy.
Answer: b
Distinguishing the various types of bowel obstruction can be difficult based on history, physical findings, and radiographic studies. The patient described has intermittent to constant pain with low volume feculent vomiting. Distension is marked and progressive, and tenderness is diffuse. This scenario most likely fits with an open-loop distal small bowel obstruction. The feculent vomiting suggests a more distal rather than proximal obstruction. The lack of severe pain and signs of peritoneal irritation suggests that a closed-loop obstruction is unlikely. A colon obstruction with an incompetent ileocecal valve would be another alternative to consider if gas in the colon had been seen on x-ray.
Answer: d
There have been multiple attempts to use common clinical laboratory test criteria to identify the likelihood that obstruction is associated with strangulation. In most cases of simple obstruction, laboratory studies do not play a direct role in diagnosis but are helpful in understanding the extent of complications such as dehydration and fluid and electrolyte abnormalities. An elevation of the white blood cell count along with fever, tachycardia, and localized abdominal tenderness is one of the “cardinal signs” for risk for strangulation. However, such an elevation is nonspecific. Similarly, metabolic acidosis may be associated with intestinal ischemia as well as evidence of dehydration and fluid loss. Elevation of BUN and other electrolyte abnormalities also represent fluid loss and dehydration. Therefore, at present there is no non-invasive rapid laboratory tests that can provide information to suggest that tissue necrosis is eminent.
Answer: a, b, c
Contrast studies such as those listed above may provide specific localization at the point of obstruction and the nature of the underlying lesion. When obstruction of the small intestine is not progressively resolving, a small bowel follow-through is indicated to confirm the presence and location of the obstruction. The history of a previous right hemicolectomy in this patient may also allow reflux through the colon to define the ileocolonic anastomosis and be able to define the site of obstruction in a retrograde fashion. The potential benefits for a CT scan include not only defining the obstruction and perhaps the nature of the lesion, but also in defining any other evidence of abdominal pathology such as metastases, ascites, or parenchymal liver abnormalities which might be present in a patient with a previous neoplasm. Although none of these tests would be contraindicated, failure of this patient to improve will likely mandate an operation and make contrast studies unnecessary. There would appear to be no evidence of strangulation or perforation therefore there are no contraindications to these studies.
Answer: d
Acute pseudo-obstruction of the colon, known as Ogilvie’s syndrome, is a paralytic ileus of the large bowel characterized by rapidly progressive abdominal distension often without associated pain. Plane radiographs of the abdomen may reveal air in the small bowel and distension of discrete segments of the colon (cecum or transverse colon) or the entire abdominal colon. Distension can become impressive, oftentimes in chronic cases distension in excess of 15 cm can be observed without evidence of colon perforation or wall ischemia. Major risk factors for the development of Ogilvie’s syndrome include severe blunt trauma, orthopedic trauma or procedures, acute cardiac events or coronary bypass surgery, acute neurologic events or neurosurgical procedures, and acute metabolic derangements. Initial management includes resuscitation and correction of the underlying metabolic and electrolyte abnormalities. A nasogastric tube is indicated if the patient is vomiting and will prevent swallowed air from passing distally. If distension is painless and the patient shows no signs of toxicity or bowel ischemia, expectant management can be successful in about 50% of cases. If distension worsens so that the cecal diameter increases beyond 10–12 cm or if it persists for more than 48 hours, colonoscopy is recommended. Endoscopic decompression is successful in 60–90% of cases, but colonic distension may recur in up to 40% of cases. Rectal tubes are ineffective in managing distension of the proximal colon, however, such tubes may be useful after colonoscopy.
Answer: a, d
Peritoneal adhesions account for more than half of the cases of small bowel obstruction in the United States. Obstruction in the immediate postoperative period following abdominal surgery, however, is uncommon, occurring in only 1% of patients in the four weeks following laparotomy. Hernias of all types are second only to adhesions as the most frequent cause of obstruction. External hernias such as inguinal or femoral hernias may present with symptoms of obstruction. Femoral hernias are particularly prone to incarceration and bowel necrosis, due to the small size of the hernia inlet. One important consideration is the Richter’s hernia. In this variant, only a portion of the bowel wall is incarcerated. These most frequently occur in association with femoral or inguinal hernias. Complete obstruction can occur if more than half to two-thirds of the bowel circumference is incarcerated. About 5% of intussusception cases occur as adults. Intussusception occurs when one segment of bowel telescopes into an adjacent segment, resulting in obstruction and ischemic injury to the intussuscepting segment. Ninety percent of adult cases are associated with pathological processes. Tumors, benign and malignant, can act as a lead point against the sussesception in over 65% of adult cases.
Answer: b
The term ileus reflects the underlying alterations in motility of the gastrointestinal tract, leading to functional obstruction. From a practical standpoint, ileus represents the interval between abdominal exploration and the reappearance of flatus and bowel movements. Distinguishing a normal postoperative ileus and the prolonged course of a “paralytic” ileus is based primarily on the time since operation and the clinical circumstances. Besides the location of the previous operation (upper abdominal, lower abdominal, pelvic., the nature of the previous operation and the findings may also contribute. Peritonitis or spillage of noxious material leads to an increase in the delay of return of normal bowel function. Distinguishing a paralytic ileus from mechanical obstruction can oftentimes be difficult. Abdominal x-rays in a postoperative ileus should reveal gas in segments of both the small and large bowel. Upper GI contrast or CT scan may also be helpful. Early postoperative obstruction is uncommon and is particularly rare for upper abdominal surgery, with most cases occurring after surgery of the colon, particularly abdominal perineal resection. There has been little success in the use of prokinetic agents to shorten recovery times after lower abdominal procedures. The use of intravenous patient controlled analgesia may delay the recovery of postoperative ileus when compared to the IM route of narcotic administration.
Answer: b, c
The principles of management of a patient with small bowel obstruction include initial fluid resuscitation and restricting oral intake. The optimal fluid for resuscitation in this patient with a distal small bowel obstruction would likely be Ringer’s lactate or normal saline. Since gastric secretion is a small component of the fluid loss, potassium replacement is likely not particularly important. An indwelling urinary catheter should be placed to monitor the urine output to reflect the fluid status. Invasive hemodynamic monitoring with a central line is likely unnecessary unless concerns are raised about cardiac status. Nasogastric decompression is indicated in all but mild cases. The nasogastric tube serves to prevent distal passage of swallowed air and minimizes discomfort of reflux of intestinal contents and eliminates vomiting. There appears to be no clinical evidence suggesting the need for urgent operation and therefore resuscitation prior to surgery is of optimal importance in this patient.
It has been well established that perioperatively-administered antibiotics reduce wound infection and abdominal sepsis rates in patients undergoing operation to relieve intestinal obstruction, simple or strangulated. Once the decision has been made to proceed with surgery, broad spectrum antibiotics, covering gram-negative aerobes and anaerobes should be given. The use of antibiotics in patients who have not been committed to operation has not been evaluated systematically. Giving antibiotics to patients who are being observed can obscure the underlying process and, in the end, delay optimal therapy.
Answer: b, c
The most common site of volvulus is the sigmoid colon, accounting for 65% of cases. The preferred method and management involves endoscopic decompression. This conservative approach resolves the volvulus in 85% to 90% of cases, and elective resection of the redundant segment can then be planned. Following endoscopic decompression, recurrence of the volvulus is higher than 60% if sigmoid resection is not performed. If the patient presents with peritoneal findings, sepsis, and shock, rapid resuscitation followed by urgent resection and colostomy is warranted.
Answer: b, c
A common manifestation of Crohn’s disease is perianal disease, including anal fistulas with extension into the adjacent organs and soft tissue regions, fissures, and perirectal abscesses. The prevalence of perianal disease approaches 25% for patients with ileitis, 50% for ileocolitis, and 40% for those with isolated colonic involvement. Perianal disease is one of the initial signs of presentation in one-third of patients. Although broad spectrum antibiotics are clearly indicated for septic complications of Crohn’s disease, their use as a primary treatment has generally been met without success. Metronidazole has been used effectively in the treatment of perianal disease. In general, a conservative surgical approach to perianal disease is usually prudent. Many patients who have indolent anal fistulas can live comfortably with their disease for years. Although the development of an abscess requires conventional drainage depending on the state of Crohn’s involvement of the rectum, standard surgical procedures can be applied to most forms of perirectal and perianal disease. Proctectomy may be indicated for patients with advanced perianal disease in direct continuity with active rectal involvement.









